Carbon & environmental data management without compromise.
Software that’s configured to the way your business really works.
Map your unique carbon & environmental inventory to streamline, unify, and automate the flow of data across your entire business and beyond. Delivering granular carbon & environmental metrics that unlock insightful decision-making & always-on compliance.

















Benefits
Works with any data
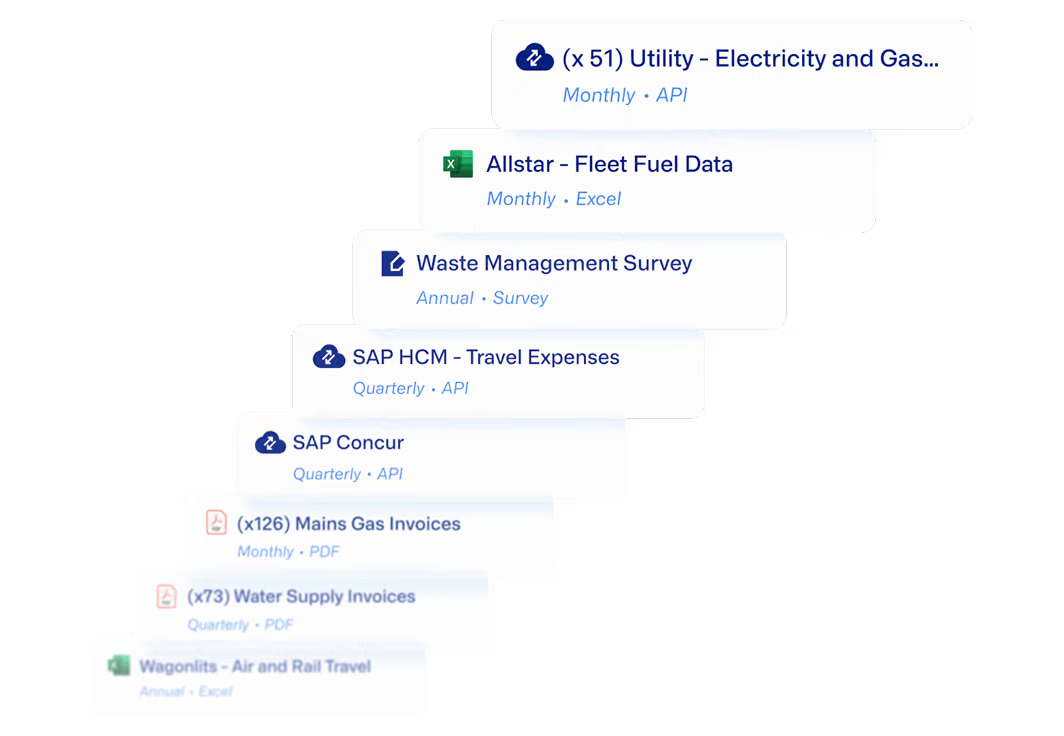
Get the carbon & environmental data outputs you need without changing your data or processes. Minimum seamlessly ingests data from wherever it lives without any manual processing or wrangling from your teams.
Whether it’s a PDF scan, an Excel file, an automatic utility provider connection, or an integration with your existing IT systems, the system ingests, processes, and verifies all your existing data automatically.
Capture any detail of your organization
Fully map your carbon & environmental inventory by capturing all assets, activities, sites, business units, regional allocations, sub-meters, and more. Use multiple taxonomies simultaneously for analysis purposes, while always staying compliant with carbon reporting aggregation standards.

Automate data workflows while maintaining quality & trust
Avoid “garbage-in, garbage-out” by applying variance checks, approval workflows, and governance policies to the data that’s entering the system. Centrally manage data flow to provide total control over the data ingestion process — on an annual, quarterly, monthly, or weekly basis.



How it works
It’s easy to get started with Minimum. Whether you’re transitioning from Excel, from an existing solution, or if this is your first time gathering environmental and carbon data: Our expert team is here to support you and configure our software to your precise needs to ensure your ongoing success.


Create a plan to capture all aspects of your organization and inventory. Both now and in the future.

Define your data submitters and approvers. Configure collection methods, cadence and controls.

Expert guidance to train your data submitters, support data completeness and enable variance checking.

Access the platform on an ongoing basis to collect data, access footprint insights, generate reports, and see your audit trail.

Work together to improve data quality, frequency and completeness. Generate more precise and actionable insights.

No more compromising on environmental data
There’s a revolution happening with Environmental data. What worked a few years ago — an annual high-level picture of the Scope 1-3 footprint, built on flaky data and underpinned by a patchy audit trail — is now woefully inadequate for what we need in 2025. Corporates need to fuel iron-clad disclosures, impactful decarbonisation, and deep insights into the opportunities and risks presented by a changing climate.
At Minimum, we’ve built software that specifically solves the data challenge for large Enterprises through a laser focus on excellence in those three areas: deep & dynamic inventory mapping, hyper-flexible data ingestion (internal & across the value-chain), and powerful auditable calculations.
And by doing that, we create a constant stream of high-quality data that can power iron-clad Sustainability & ESG reporting and genuine progress against decarbonization targets.
If you’re a large business looking to invest in a genuinely powerful quantitative environmental data management capability to drive your sustainability agenda for years to come — please get in touch. We’d love to show you environmental data without compromise.
Decisions need to be made on data that’s weeks old, not months old. Data processing needs to be automated & scalable without compromising on quality. Every number needs to stand up to scrutiny. Metrics & insights need to be precisely tailored to the specific operating model of the business. Data needs to be available across the entire organisation. And Sustainability practitioners need to be freed from the toil of carbon accounting so they can focus on driving change. Modern Enterprises face constant pressure from customers, investors, regulators, governments — they need a data system that can help them withstand this pressure.
There are three parts to solving this data challenge: inventory mapping, data ingestion & calculation. Three things that are simple to write but incredibly hard to achieve for businesses operating at any significant scale — and they need to be done extremely well. The inventory has to be mapped at an extremely granular level, capturing the nuance of operations, and be reactive to constant changes as the business evolves. Data inputs are disparate, messy, and patchy — involving internal and external stakeholders. And the resulting data has to be more frequent, wider-ranging, more intricate, more trustworthy, more insightful, than ever before.

Environmental data capabilities to power your sustainability agenda
Minimum provides you with the foundational capabilities that can underpin your climate and sustainability programme for years to come. Click each capability to learn more.
Minimum’s Carbon Atlas™ is a flexible system for mapping and managing environmental inventories across large organizations. It handles complex corporate & operating structures and gives you a clear picture of how your inventory is configured and how data is gathered, transformed, and validated.
Automate data ingestion from all sources while staying in control through powerful variance checking & approval workflows.
Minimum’s calculation engine, emissions factor database, and core data model is compatible with the GHG Protocol and all major carbon accounting and ESG reporting requirements.
Minimum gives you reporting confidence and practical insights from your environmental data — so you spend less time reporting and more time driving improvement.
Minimum is designed to flexibly connect to your existing technology stack, making environmental data flow effortlessly between systems.
Minimum’s calculation engine, emissions factor database, and core data model is compatible with the GHG Protocol and all major carbon accounting and ESG reporting requirements.
Automate data ingestion from all sources while staying in control through powerful variance checking & approval workflows.
Minimum makes environmental data collaboration simple, controlled, and transparent—both internally and across your wider value-chain.
Inventory mapping
Data ingestion
Calculations
Reporting
& insights
Integration
Auditability
Governance
Collaboration & engagement
Project management & control
Data security



Dig a little deeper
Stay ahead of the curve with deep industry analysis, practical guides, and insights from our environmental data experts. Discover how leading organizations are structuring their environmental data to achieve compliance, drive decarbonization, and make better business decisions.



